




An overview of Herpes Zoster Ophthalmicus | Lesson
Introduction
Herpes Zoster Ophthalmicus (HZO), is a viral disease caused by the reactivation of the Varicella Zoster Virus (VZV), which commonly causes chickenpox, and typically presents in mid to late adulthood. It is, in essence, ‘shingles’ of the face and eye and is characterised by a painful, unilateral vesicular rash distributed throughout one or more of the dermatomes of the trigeminal nerve. The trigeminal nerve provides sensory innervation to the eye and its structures, as well as providing some sympathetic input. Owing to this shared innervation, the eye and its components lie at risk of viral infiltration leading to potential vision-threatening complications which develop over days to months.1
Aetiology
VZV is the herpes-virus responsible for chickenpox, an infection which occurs typically in early childhood. When this primary infection resolves, the virus lies dormant in the dorsal root ganglia of the spine in the case of most dermatomes which may be affected.2 When the virus reactivates, it presents in the form of HZ.
HZO is a descriptor for the development of HZ in the distribution of the trigeminal nerve (cranial nerve V) specifically (Figure 1). The aetiology is the same in HZO apart from the fact that the VZV reactivates via the sensory ganglia of CNV as the cranial nerves lack a dorsal root ganglion.1
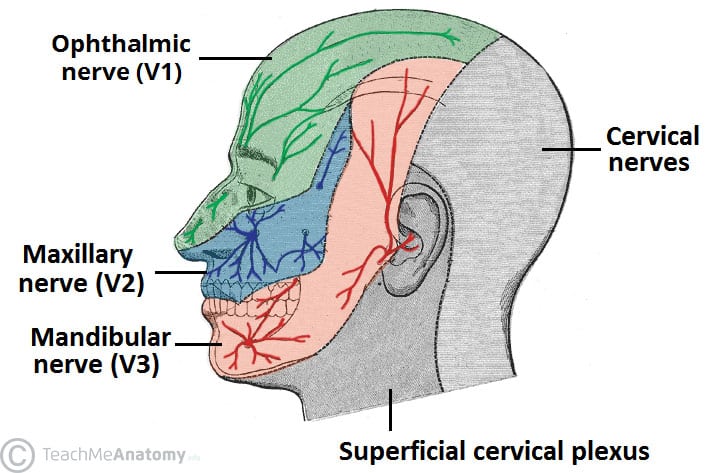
Figure 1: Dermatomal distribution of the trigeminal nerve3
Epidemiology
HZ’s prevalence incidence steadily increases with age, its rates doubling between the ages of 25 and 60 years. The reactivation of VZV is largely driven by a reduction in cellular-related immunity associated with ageing and states of immunosuppression.2
HZ rates vary by age, with 1.2-3.4 cases per 1000 in younger populations and 3.9-11.8 per 1000 in adults aged over 65 years old.2
HZO accounts for approximately 10-25 per cent of all cases of HZ, a significant proportion of the yearly millions of HZ cases globally.
Incidence rates vary by ethnicity, with Caucasian individuals experiencing the highest rates and lower rates seen among those of African and Asian descent.1
Risk factors
As evidenced by the epidemiology of HZ, the major risk factors for its development, and thus the development of HZO, are those of increasing age and immunocompromise.
Immunosuppression via malignancy, transplantation, or HIV, for example, lead to notably severe, resistant, or recurrent presentations. HZO manifests commonly in patients with HIV/AIDS, seen in roughly one-in-five patients.1 In cases of severe or unresolving HZO with no clear source of immunosuppression, HIV serology should always be arranged and its management is crucial not only to the treatment of HZO, but to the quality and length of the patient’s life.
Immunosuppression predisposes patients to the development of rarer and more severe complications of HZO such as acute retinal necrosis (ARN), optic neuritis, and panuveitis among others,1 and should be borne in mind by the treating clinician when dealing with an immunosuppressed patient. Not only are these rare complications more likely, but they also tend to progress more rapidly and result in worse outcomes.
Other weaker risk associations include female sex, physiological stress, ethnicity, and co-morbidities such as diabetes mellitus, autoimmune disease, and renal disease.
Presentation
HZO classically presents as a painful, unilateral, vesicular rash with a dermatomal distribution. Its clinical course, as with HZ eruptions in all areas of the body, is divided into three stages: pre-vesicular, vesicular, and post-vesicular/recovery.2
In the pre-vesicular phase clinical features commonly include neuropathic pain, usually described as a burning or tingling sensation, which will accompany and frequently precede the rash. Some individuals may experience fevers and headaches in this preceding period also. 2
The pre-vesicular phase is the ideal period of illness to commence antiviral treatment but the vague nature of the symptoms without any visible abnormality results in infrequent attendance at this point.
Over the following two-to-three days the classical herpetic vesicles will appear, marking the start of the vesicular phase. These blisters will weep, crust over and eventually heal.
In the context of HZO, extension of the rash to the tip of the nose, known as Hutchinson’s sign (Figure 2), indicates the involvement of the nasociliary branch of the ophthalmic branch of the trigeminal nerve shared by the ocular structures and represents an increased risk of ocular involvement and complications.1
The post-vesicular phase and recovery from HZO can last many months. HZ breakouts are considered chronic when the associated pain lasts for over four weeks.2 In cases of HZO, the virally-mediated ocular manifestations present over the course of days to months and require follow-up and surveillance.

Figure 2: Unilateral vesicular rash of HZO which also demonstrates Hutchinson’s sign by its extension to the nose.4
Ocular manifestations
Ocular involvement in HZO affects approximately half of patients, and has the potential to affect every structure of the eye, and results in a range of outcomes from irritation to permanent and severe vision loss.1
Viral infection and inflammation of the eye typically begins anteriorly and progresses with time towards more posterior structures. The anterior elements of the eye consist of the conjunctiva, cornea and anterior chamber (Figure 3). The eyelids may also be affected.
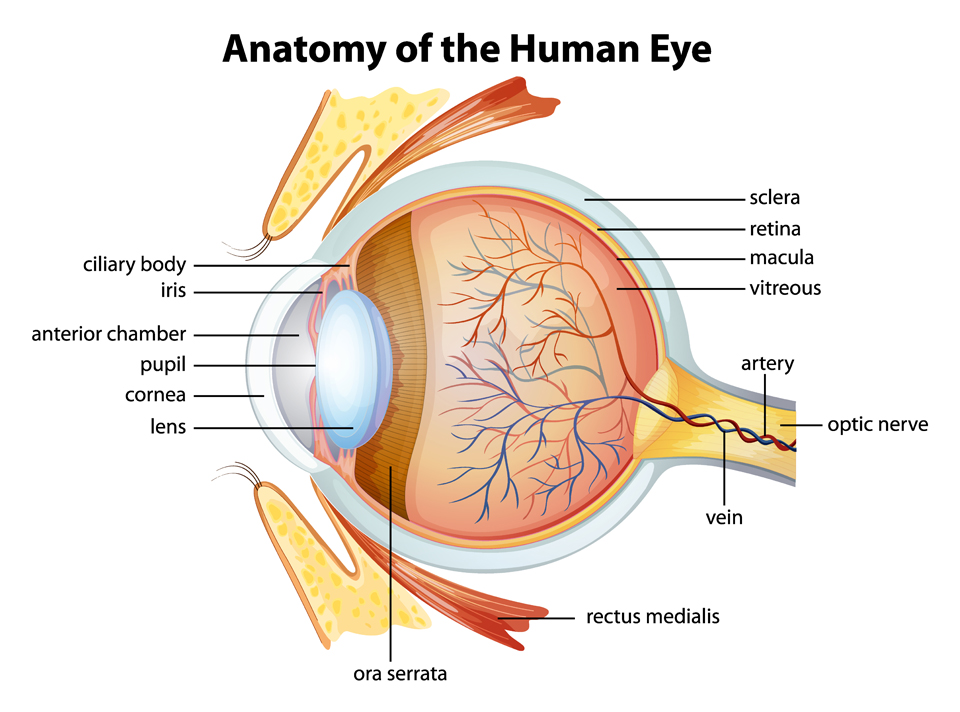
Figure 3. Anatomy of the eye5
This initial stage of inflammation may become apparent within one-to-two weeks of HZO onset and presents with hyperaemia, irritation, and watering of the eye. The eyelids and conjunctiva may additionally be affected by vesicles alongside the skin.
A viral conjunctivitis, scleritis or episcleritis may develop, all of which can lead to chronic complications such as scarring of the surrounding skin and conjunctiva, resulting in chronic dry eye, which can severely impact on patient quality of life and comfort.
Keratitis is one of the most common ocular manifestations of HZO, with disease beginning in the epithelium and progressing deeper into the structures of the cornea over time if not adequately recognised and treated. Infiltration may begin in the anterior stromal layer within one-to-two weeks, with deep stromal keratitis taking up a year to develop. The occurrence of a deep stromal keratitis risks the infiltration of the virus into the anterior chamber, resulting in uveitis.1,6 Its appearance under fluoroscopy morphs as it develops. It begins as a superficial punctate pattern and develops into a characteristic and easily recognised pseudodendritic pattern (Figure 4). These pseudodendrites differ in appearance to true corneal dendrites seen in primary HSV infection of the eye,1,7 though the distinction is not of great importance as the presence of either should prompt immediate referral to an ophthalmologist.

Figure 4. Pseudodendrites8
Complications specific to keratitis include neurotrophic keratopathy marked by reduced corneal sensation of the eye. This has the potential to lead to corneal ulcers which may go unnoticed by the patient. If not addressed in time, they can become a chronic issue with potential for bacterial superinfection and clouding of the cornea leading to blindness.6 If disease is allowed to progress to this point, the only curative treatment is corneal transplantation.1
Anterior uveitis can occur alone or in combination with keratitis. Its onset is most typically two-to-four weeks after onset of HZO. Uveitis commonly drives inflammation of the trabecula, impeding the outflow of aqueous humour and increasing intraocular pressure, which if left untreated, leads to glaucoma.7 Symptoms to be aware of include blurring of vision, ocular pain, and headache.
The posterior segment of the uvea may rarely be affected by ARN, which manifests as patches of retinitis that merge and presents as acute onset vision loss in one eye, redness, photophobia, and floaters, like the presentation of retinal detachment, which often also occurs.1,9 As previously mentioned, it predominantly presents as a manifestation in the immunocompromised.
Complications
- Vision loss: Some degree of visual loss may be seen in up to 20 per cent of HZO patients, with severe and total visual loss being rarer. Visual loss is most associated with uveitis, with more severe and total loss being associated with immunosuppression, baseline visual acuity, and older age.1 Just as a positive Hutchinson’s sign increases the risk of ocular involvement in HZO, it also increases the risk of vision loss.
- Recurrent or chronic disease: Up to 25 per cent of patients will experience recurrence of HZO at least once.1 Frequent recurrence may be associated with a significant psychological burden along with economic impacts owing to the painful and visible nature of the rash. Additionally, each recurrence risks similar eye involvement as the previous and all the accompanying complications. Patient education and antiviral therapy as soon as possible is key to management and patients should be given a back-up prescription to keep at home in the case of further outbreaks.
- Post-herpetic neuralgia: A potentially disabling complication in which the nerve pain associated with HZ persists beyond resolution of the vesicles. Allodynia and hyperalgesia are common and the pain itself is often refractory and requires a combination of both oral and topical medications to treat, which itself can be a challenge due to side-effects.2,10
- Glaucoma: This is a common complication arising from HZO uveitis. As mentioned previously, inflammation and swelling of the trabecula leads to impeded outflow of the vitreous humour, resulting in increased intraocular pressure and glaucoma development.
- Scarring of the cornea: Secondary to keratitis.
- Secondary bacterial infection: Particularly of the cornea.
- Dissemination to encephalitis: Especially in immunocompromised patients, can also lead to more widespread disseminated zoster infection.1
- Stroke: A rare complication, caused by a combination of viral inflammation leading to vasculitis and a pro-thrombotic state.7
Differential diagnosis
Other diseases may mimic HZO. These may broadly be broken down by focusing on conditions with similar rashes, conditions with similar pain, and conditions with similar ocular findings.
Pain differentials:
If facial pain and neuralgia is the primary complaint with no evidence of a vesicular rash, then the following must be out ruled as causes:
- Migraine: Similar in that their pain is unilateral, however, the timeline of pain is shorter and they may be accompanied by a preceding aura.
- Cluster headache: These headaches are defined by short bursts of excruciating facial pain. Several will usually occur over the course of weeks hence the term ‘cluster’.
- Compression of the trigeminal nerve: Defined by episodes of intense shooting or shock-like pain that are triggered by often as little as tooth brushing or speaking.
- Giant cell arteritis: Defined by tenderness over the temporal region.
Rash differentials:
HZO, by definition, will not cross of the midline of the patient’s face and if it does so an alternative diagnosis should be considered.
Important differentials to consider for similar vesicular rashes include:
- HSV infection: An important differential. The main difference in presentation will be the pattern of vesicles – small clusters which may cross the midline as opposed to a rash throughout the dermatomal region.1 As both conditions are caused by viruses from the herpes family there is commonly a similar prodromal pattern and pain symptoms.
The history may offer insight into differentiating between the two – in the case of HSV infection there may be a history of recent cold sore infection or contact as a source of infection. Regardless, treatment remains the same and of great importance as similar eye disease and complications can occur as do in HZO.
- Primary VZV infection: Will have a more widespread distribution and potentially a contact history.
- Contact dermatitis: History of use of a new detergent, cosmetic, etc, in the region and will likely lie outside a dermatomal distribution based on use history.
- Impetigo: will not conform to a dermatomal distribution, will have a less vesicular appearance though may crust over similarly.
Ocular differentials:
All the below have been described above, and in the case of clinical doubt should be referred to ophthalmology:
- Conjunctivitis
- Episcleritis/scleritis
- Uveitis
- Glaucoma
Early recognition, diagnosis and referral
HZO is broadly a clinical diagnosis. PCR swabs can be sent to the lab in cases of diagnostic uncertainty but should not delay treatment or referral in cases of high clinical suspicion.1
Presumed HZO should be referred early to an ophthalmologist to help reduce the risk of vision-threatening outcomes. Ideally all cases should be referred and seen, however, cases which present with Hutchinson’s sign, conjunctival/ciliary pain, conjunctival injection, changes in vision, or abnormal eye movements on exam should be prioritised for referral as these signs indicate a higher likelihood of ocular complications.1
Treatment
Equally important to early recognition is early and effective treatment of HZO. Prompt use of antivirals, particularly in the pre-vesicular phase, reduces the length and intensity of the outbreak as well as reducing the chance of ocular infection and complications, both visual and non-visual. One study demonstrated a reduction in chronic ocular complications of 40 per cent in those who were treated early with antivirals highlighting the importance of decisive management.1
Treatment with antivirals should ideally begin within the first 72 hours of illness, though beginning treatment after this window is still valuable, particularly in cases where there is ongoing creation of new vesicles.11 Many clinicians will recognise the difficulty of practising and prescribing within this window, as less than 50 per cent of patients with HZO will present within three days of symptom onset,1 adding another layer of complexity in the management of this condition.
Antiviral treatment regimens vary but the most common are as follows:
- Acyclovir 800mg five times daily for seven days
- Famciclovir 500mg three times daily for seven days
- Valacyclovir 1000mg three times daily for seven days11
Although more expensive, patient preference may guide the prescription of the latter two due to the less frequent dosing regimen and likely increase in medication compliance, which is essential to effective treatment. Ocular complication rates have been shown to be similar across these three options and thus the choice lies in clinician and patient preference.1
In patients who are immunocompromised, IV acyclovir in the hospital setting may be preferred and in cases of acyclovir-resistant infection, IV foscarnet may be used.1
There is currently no strong evidence to support long-term antiviral therapy with a view to prevention of longer-term ocular complications. The ZEDs trial has been the only trial to measure this across time and demonstrated non-significance for overall occurrence of complications with antiviral treatment over the course of a year following HZO versus placebo.12
Supportive measures such as appropriate analgesia, ocular lubricants, and topical corticosteroids are essential. Topical corticosteroids are effective at reducing inflammation of the eye, yet they must not be used prior to commencement of antiviral therapy and ideally should be prescribed by a specialist. Steroids dampen the body’s natural immune reaction, and their use without antiviral medication gives the virus free rein to proliferate and spread, leading to increased risk of complications, particularly acute retinal necrosis, although the overall risk remains low.1
Follow-up visit frequency is based on presence or absence of ocular involvement. In eye-sparing disease, follow-up at 10-14 days is appropriate.1 In cases with ocular involvement, initial follow-up is more frequent and varies based on clinical judgement, ongoing follow-up at six–12-month intervals follows to screen for further late complications.13
Prevention
Prevention of HZO is dependent on the general prevention of HZ infection. This is now possible with the introduction of effective vaccination. Shingrix, a recombinant vaccine now available on the Irish market, has demonstrated a prevention rate of 97 per cent in those >50 years old and 91 per cent in those over 70 years old (ZOE-50 and ZOE-70 phase 3 trials).14,15 Meta-analysis has shown Shingrix to have a prevention efficacy of 88 per cent against HZO formation.1
Vaccination is recommended for those aged over 50 years and those over 18 years who are immunocompromised.16 However, at present, the vaccine is not available through the HSE and must be paid for privately (costing more than €400 for a course of two vaccines), which is prohibitively expensive for many. Nevertheless, GPs and practice nurses play a vital role in recognising patients who are eligible for vaccination, and prompting a discussion with them regarding its benefits, with room for expansion of this role if the vaccine becomes reimbursable.
Summary
In summary, HZO represents a potentially vision-threatening clinical entity. It is characterised by a painful vesicular rash across the distribution of the trigeminal nerve and risks ocular involvement throughout all the structures of the eye. Its outcomes range from temporary pain and discomfort to vision loss in the eye. Early recognition, referral and treatment are essential to prevent permanent damage to the eye. Prevention of HZO occurrence through appropriate vaccination in at-risk populations is our best treatment and will likely become an increasingly important part of tackling this condition in the future.